
Finger Pulley Injuries and the Value of Taping

By Chris Fletcher
We have all seen some gnarly fingers from seasoned Jiu-Jitsu practitioners and have probably felt the pain of a powerful grip break. This is one place where taping fingers is a benefit: to decrease risk of injury, to help rehab an injury, and to decrease the pain of osteoarthritis.
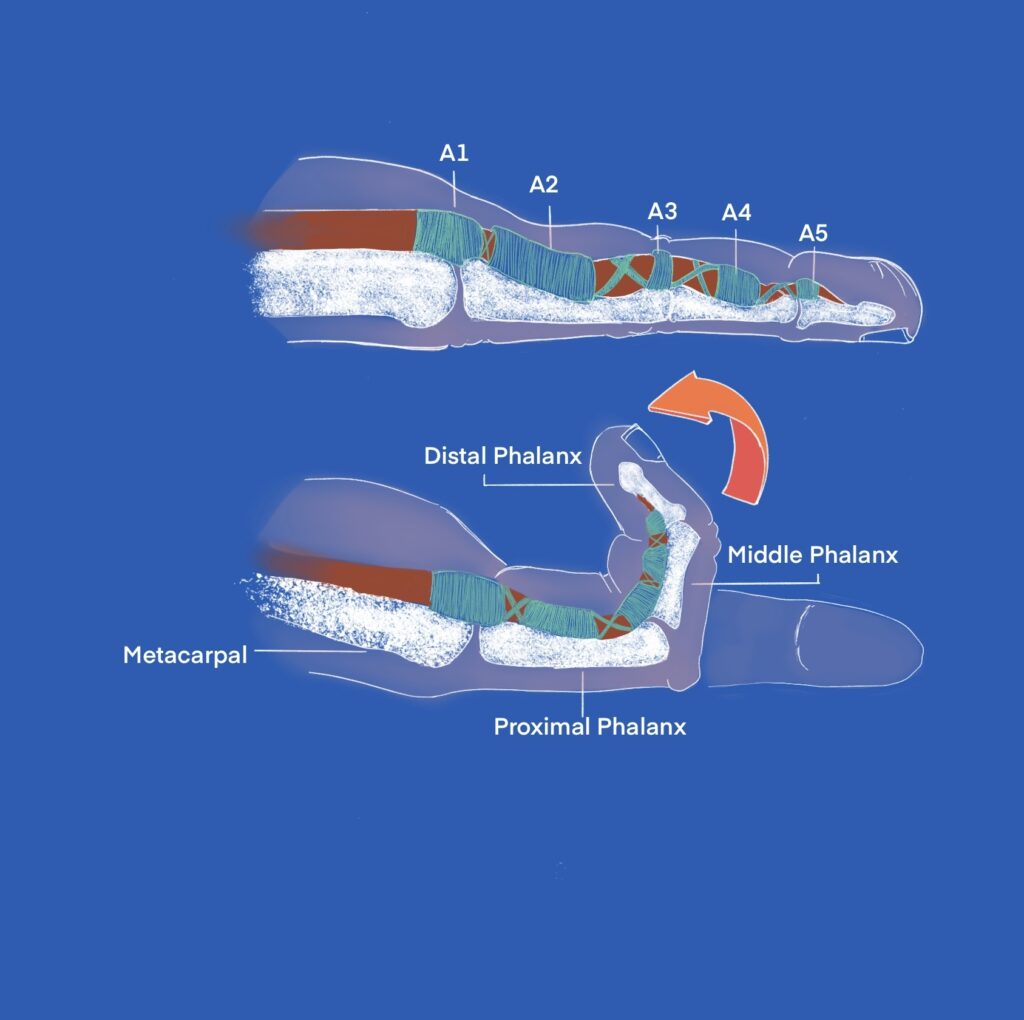
There are three regions of the hand: the wrist is made up of the carpals, the palm is made up of the metacarpals and the fingers are made up of the phalanges. The pulley system is on the palm side of the phalanges and made up of five pulleys named A1-A5, pulleys are specialized structures that hold the flexor tendons close the the bone.
Many injuries to the thumb and fingers are caused by grip making or breaking. The ulnar collateral ligament of the thumb can be sprained or torn; the ligaments in three joints that make up the fingers can be sprained or torn; the tendons can be torn off the finger bones; the pulleys that attach the tendons to the bones can be sprained or torn; and the fingers or thumb can also be fractured.
Finger flexor pulley injuries are very commonly reported in rock climbers from use of crimping, but these can also happen in Jiu-Jitsu when a grip is forcefully broken, especially pocket grips used commonly during spider guard. The flexor tendons run on the bottom side of the finger and, in order for them to stay close to the bone, pulleys are needed. The pulleys that are typically injured are the A2 and A4 pulleys. (1)
Grades of Pulley injuries
- Grade I – pulley strains
- Grade II – complete rupture of A4 pulley, or partial rupture of A2 or A3 pulleys
- Grade III – complete rupture of A2 or A3 pulleys
- Grade IV – Multiple pulley ruptures or single rupture of A2 or A3 with lumbrical or collateral ligament injury.
Imaging
Plain X-ray can be used first to rule out finger fracture or volar plate avulsion. Ultrasound and MRI are then used to differentiate between pulley strain, partial, or complete rupture. (1)
“Investing time and a little money into taping your fingers before Jiu-Jitsu can actually have long-term benefits in reducing risk of injury.”
Treatment
- Conservative
Grades I-III injuries are typically managed conservatively. Grades I and II will typically recover within six weeks but protective taping is recommended for three months. The taping is usually circular taping around the distal end of the proximal phalanx.
Grade III injuries should be splinted for 10 – 14 days, then gentle range of motion exercises and gradual return to sport in two months with full return after three months and protective taping for six months. (1)
- Surgical
Grade IV injuries usually require surgical repair. A common procedure is using a palmaris longus tendon graft and wrapping it two to three times around the phalanx. (1)
Using tape can provide protection and even prevent injury. When the last two joints of the fingers are taped, it decreases the stress on the furthest joint (DIP). This reduces the possibility of hyperextending and decreases the force on the A2 pulley, which then decreases risk for a finger flexor pulley injury. (2) Unfortunately, a different study showed that grip strength between taped and non-taped fingers and wrists were the same, so tape doesn’t improve grip strength,(3)
Investing time and a little money into taping your fingers before Jiu-Jitsu can actually have long-term benefits in reducing risk of injury and most likely reducing risk of developing gnarly osteoarthritic fingers.
Disclaimer: The content in this article is for informational purposes only – it is not intended to delay or substitute for professional medical advice, diagnosis, and/or treatment. The content is not intended to promote understanding of various musculoskeletal injuries. Content may not apply to your specific condition or symptoms. Always seek the advice of your physician or other qualified medical professional for any question you have for a medical condition.
References:
1. Reid D. The management of greater trochanteric pain syndrome: A systematic literature review. J Orthop. 2016 Mar; 13(1): 15–28.
2. Flack N, Woodley SJ, Nicholson HD. Fiber type composition of the hip abductor muscles. Anatomy. Feb 2021.
3. Cowan RM, Semciw AI, Pizzari T, Cook J, Rixon MK, Gupta G, Plass LM, Ganderton CL. Muscle Size and Quality of the Gluteal Muscles and Tensor Fasciae Latae in Women with Greater Trochanteric Pain Syndrome. Clinical Anatomy. Volume 33, Issue 7, Oct 2021.

Our printed magazine is full of extraordinary women with extraordinary stories, get your printed copy via mail today >
 Return to Play
Return to Play  Hypermobility Spectrum Disorder
Hypermobility Spectrum Disorder  Hip Pain and the Sneaky Tensor Fasciae Latae
Hip Pain and the Sneaky Tensor Fasciae Latae  Low Back Pain
Low Back Pain  Toe Hold
Toe Hold  Wrist Locks:
Wrist Locks:  Father Time is Undefeated
Father Time is Undefeated  The Jiujiteira Sisterhood
The Jiujiteira Sisterhood  Advice in the Ranks- From White to Black
Advice in the Ranks- From White to Black  ADGS Rome: Jiujiteiras Shine in the Land of the Colosseum
ADGS Rome: Jiujiteiras Shine in the Land of the Colosseum